Association of Individuals’ Chronotypes With Obesity and Body Composition in Tehrani Adults in 2020
Article information

Abstract
Objective
Individual’s preferences in time for sleeping, waking up, doing physical and mental activity is dependent on chronotypes. According to these preferences, individuals are categorized to morningness, intermediate, and eveningness chronotype. Recently, it has been suggested that chronotypes are involved in regulation of sleep, appetite, and some metabolic factors. The aim of this study was to investigate the association between chronotypes, obesity, body fat, and lean mass in Tehrani adults.
Methods
It was a cross-sectional study on 353 adults aged 18–60 years who referred to Tehran community centers. After anthropometric measurements and collecting data on general information, choronotype, physical activity and 3-day food recalls, fat mass, and lean mass were measured using the method of bioelectrical impedance analysis. SPSS 21 was used to statistical analysis.
Results
Of total 353 participants, 11%, 47.6%, and 41.4% had eveningness, intermediate, and morningness chronotypes, respectively. The mean age of individuals with morningness and intermediate was higher than those with eveningness. The prevalence of eveningness in men was higher than in women (p=0.001). Fat mass and lean mass in individuals with eveningness type were higher and lower than those with morningness, respectively (p<0.05). Body mass index and waist circumference showed no significant difference among chronotypes.
Conclusion
Eveningness type is associated with increase in fat mass and decrease in lean mass. The effects of chronotype on body fat and lean mass are independent of obesity.
INTRODUCTION
People have distinct individual differences in their chronotypes. One of the most important differences is the morningness-eveningness preferences or the chronotype. The difference in the preferences of the time of sleep and wake up as well as the preferences of the time of physical and mental activity in different people depends on their chronotype. Accordingly, people are classified into morning type, evening type, and intermediate type [1]. People naturally have morning type. By awaking and exercising out of daylight hours, the body’s biological rhythm losses its normal phase [2]. Thus, evening type typically is associated with loss of synchronization between the biological and the peripheral clock. In modern societies, lifestyle changes and increase in working hours, especially night shifts, have affected food patterns. The results of some recent researches suggest that the evening type and late consumption of meals are associated with obesity. Being awake during the night, such as what is seen in night shift staffs and people with evening type, can lead to increase in appetite and higher food intake and consequently, obesity [3]. There is evidence that the loss of coordination between the biological clock and the peripheral clock leads to a disturbance in the regulation of energy balance. In such a way that calorie consumption in dark (rest or inactive) phase may be associated with obesity [4,5]. Some researches have shown that food consumption in unusual times, such as what is seen in people with the evening type, may disrupt the body’s normal metabolism [6]. Studies in mice have shown that eating during daylight hours is associated with normal metabolism, while eating in dark hours, leads to metabolic disorders and some chronic diseases such as obesity and diabetes. Therefore, eating equal amounts of food during the day may have different effects on body weight compared to eating at night [7]. One of the effective mechanisms can be attributable to the variation of the effect of diet induced thermogenesis (DIT) during day and night. DIT has the highest value in the morning, then decreases in the afternoon and evening, respectively [8]. Another mechanism may be related to changes in serum leptin levels. This means that eating at unusual hours leads to overeating, which is partly due to the malfunction of appetite regulation systems. Considering that the body’s circadian clock controls the expression of the leptin gene as an appetite suppressive hormone, disruption to the order of this clock leads to reduction in serum leptin during the day [9,10]. Recent researches suggest that circadian chronotype, metabolism, and nutrition are closely related [11]. However, the effect of chronotype on metabolism has not yet well known. Understanding the potential physiological mechanisms due to dysregulation of awakening and eating time is critical to developing effective treatment strategies for prevention and management of obesity. According to our research, no study investigated the association of chronotypes with anthropometric measurement and body composition in Iran, so far. Therefore, for the first time, the present study investigated the association between different chronotypes with anthropometric measurement, body fat mass and muscle mass.
METHODS
Participants
This descriptive-analytical cross-sectional study was conducted on 353 men and women aged 18 to 60 years who referred to Tehran Municipality community centers through convenience sampling method. For the purpose of considering the economic situation, community centers were selected randomly from 5 regions in the north, south, west, east, and center in Tehran. Professional athletes, people who followed weight loss or weight gain diets, special diets such as vegetarian diet, traditional medicine and homeopathy from the last two months to the beginning of the study, and also pregnant and lactating women were not included in the study. During the study, participants whose energy intake was less than 800 or more than 4,200 calories per day were excluded from the analysis. The present study was approved by the Ethics Committee of National Nutrition & Food Technology Research Institute, Shahid Beheshti University of Medical Sciences (IR.SBMU.nnftri.Rec.1398.025). Before collecting data, the aims of the study were explained to the participants and after signing the informed consent form, they entered the study.
General information
For all participants, a general information form including questions about age, marital status, occupation, appetite suppressants and weight-loss drugs or supplements, antidepressant drugs, smoking in the past month, and meal time were completed.
Anthropometric measurements
Anthropometric measurements were performed by two trained dietitian. Weight was measured by a Beurer digital scale with a minimum of clothing with an accuracy of 0.1 kg and height was measured by a tape measure, without shoes and using a meter fixed to the wall with an accuracy of 0.1 cm. Waist measurement was performed by a tape meter with an accuracy of 0.5 cm in the lowest measurable environment and at the end of natural exhale, according to WHO protocol. For some people, because of obesity or malnutrition, it was not easy to measure the minimum waist circumference, the circumference of the last vertebrae was measured, because for these people, the minimum waist circumference is in this area.
Measuring body composition
To measure the percentage of body fat and lean mass, participants were asked to be attended to the diet therapy clinic of Shahid Beheshti University of Medical Sciences on the appointed day after 12 hours of fasting to measure their body composition by bioelectrical impedance analysis.
Assessment of chronotypes
The Morningness-Eveningness Questionnaire (MEQ) prepared by Horn and Ostburg [12] was used to assess the chronotypes and this questionnaire is the most common questionnaire for assessing the chronotypes. The Persian version of this questionnaire has been validated by Rahafar et al. [1]. According to their study, the Persian version of this questionnaire has acceptable validity and reliability for measuring chronotypes (Cronbach’s alpha coefficient 0.77). This questionnaire consists of 19 questions. MEQ scores range from 16 to 86. Getting higher score shows more probable for being morningness. Individuals are categorized according to getting score as below: 16–30, definite eveningness; 31–41, intermediate eveningness; 42–58, intermediate; 59–69, intermediate morningness; 70–86, definite morningness.
Assessment of food intake
To assess people’s food intake, the three-day food recall questionnaires were collected during three non-consecutive days in a week. Participants were asked about all the meals and snacks eating during the day. The dietary intake data were then converted to daily grams of food intake using household measures. Nutritionist IV software (First Databank, San Bruno, CA, USA) was used for dietary intake analysis. Then the calories received from each macronutrient and each meal were calculated separately.
Assessment of physical activity
To assess physical activity, International Physical Activity Questionnaire (IPAQ) was used. The Persian version of this questionnaire was validated by Vashghani et al. [13]. According to their study, this questionnaire has acceptable validity and reliability (0.33 and 0.7, respectively). The IPAQ used in the present study is the long interview-administered version (27 items) which covers 4 domains of physical activity including: occupational (7 items), transportation (6 items), household/gardening (6 items), and leisure-time activities (6 items). The questionnaire also includes 2 questions about the time spent on sitting as an indicator of sedentary behavior. The number of days per week and the time spent on walking per day as well as intermediate and vigorous activities from all 4 domains are recorded [11]. The IPAQ data are converted to metabolic equivalent (MET) scores by multiplying the number of minutes dedicated to each activity class by the specific MET score for that activity.
Statistical analysis
SPSS software version 21 (IBM Corp., Armonk, NY, USA) was used for statistical analysis of data. To determine the normality of the data, we used the Kolmogorov-Smirnov test. The distribution of qualitative variables was examined based on chi-square test. One-way analysis of variance (ANOVA) was used to examine the mean distribution and standard deviation of anthropometric indices, body fat, and lean mass among different chronotypes. In all tests, p<0.05 was considered as a significant level.
RESULTS
The participation rate was close to 100% in our study (99.4%). The participants’ chronotype was divided into three categories based on MEQ points: eveningness, intermediate, and morningness. The prevalence of eveningness, intermediate, and morningness type was 11%, 47.6%, and 41.4%, respectively. Of total of 353 participants, 85.8% were women and 14.2% were men. The prevalence of intermediate type in women was higher than in other two chronotypes; while in men, morning type had the highest prevalence (p=0.001). The mean age of the participants was 42.2+11.8 years. As shown in Table 1, the mean age of people with eveningness type was 37 years, intermediate type was 40 years, and morningness type was 46 years, and the mean age of people with morningness type was significantly higher than eveningness and intermediate type (p<0.001). There was no significant difference in term of work shift among three chronotypes. The frequency of people who used weight and appetite control drugs was 55%, 40% and 5% in morningness, intermediate, and eveningness type, respectively. It did not have any significant difference among three chronotypes.

Distribution of general characteristics among three chronotypes
Table 2 shows the distribution of anthropometric measurements among three chronotypes by ANOVA test. Due to the abnormal distribution of height variable, Kruskal-Wallis test was used to compare between different types of chronotype. The mean percentage of body fat mass in people with eveningness type was significantly higher than morningness type (p<0.001). In addition, the percentage of lean mass in people with morningness type was significantly higher than in people with eveningness type (p<0.001). Mean weight, waist circumference, and body mass index (BMI) were higher in the eveningness type than in the intermediate and morningness type, but they were not statistically significant.
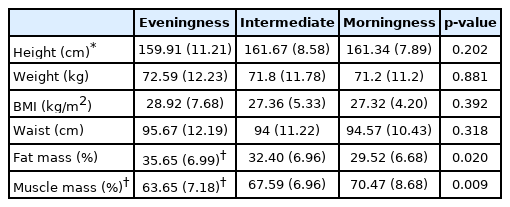
Distribution of anthropometric measurements among three chronotypes
Figure 1 shows the percentage of calories intake of each main meal from the total daily calorie intake among the three chronotypes. The percentage of calorie intake from main meals was not significantly different among three chronotypes.
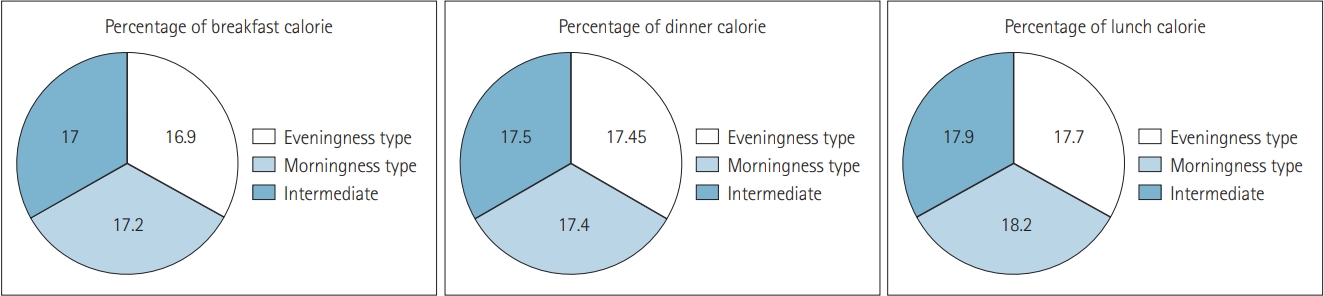
Percentage of calorie of each meal from total calorie, among the three chronotypes.
Figure 2 shows the meal time for participants with different chronotypes. Meal time for breakfast, lunch, and dinner was significantly later in eveningness type than in morningness type. Dinner time in morningness participants was earlier than in intermediate type.
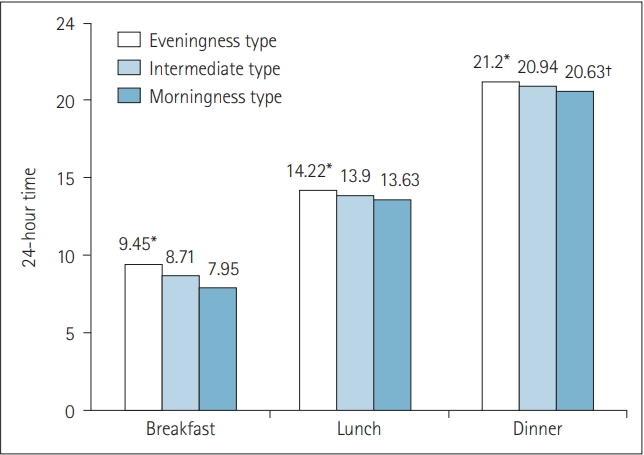
Comparing meal time among three chronotypes. *significant difference with the morningness type; †significant difference with the intermediate type.
DISCUSSION
The present study assessed the prevalence of morningness, intermediate, and eveningness chronotypes in Tehranian men and women. The intermediate type had the highest prevalence (47.6%) and the eveningness type had the lowest prevalence (11%) in the study population. The distribution of chronotypes in our study is similar to the study of Seyedoshohadaee et al. [14]. In their study, the prevalence of intermediate, morningness, and eveningness chronotypes in nurses who working in medical centers affiliated to Tehran University of Medical Sciences was 57.9%, 36.1%, and 6%, respectively. Also, in the study of Issazadegan et al. [15], the prevalence of morningness type was similar to our study (41%), the prevalence of intermediate type was slightly lower than our study (44%), and the prevalence of eveningness type was higher than ours (15%); but overall, our findings followed a similar trend. Our findings are to some extent similar to study of Bakhshandeh et al. [16] conducted on dormitory residents women which showed that intermediate type has the highest prevalence; however, the morningness type had the lowest prevalence. The results of the study by Tonetti et al. [17] also shows that the intermediate type had the highest prevalence among chronotypes; but the prevalence of morningness and eveningness type was almost equal. Part of this differences can be due to differences in general characteristics like sex, job, and lifestyle in different studies. The higher percentage of men with morningness type compared to other two types in the present study may be due to the need for men to wake up in the early hours of the morning to be at workplace. While there is no such necessity in women who participated in our study, because of the high percentage of housekeeper. On the other hand, according to the results of the present study, the incidence of morningness type increases in people with increasing age; the mean age of people with the morningness type is significantly higher than the eveningness type, which may be due to differences in the lifestyle of young people from middle-aged and elderly people. All our participants had overweight, regardless of their chronotypes. There was no significant association between BMI, waist circumference, and chronotypes. Although the mean waist circumference was higher in the eveningness type than morningness type, this was not statistically significant. Lack of significant association between chronotypes and BMI has been found in many other studies, similar to ours [18]. Such finding is not so unexpected, considering that there was no difference in terms of physical activity and calorie intake among three chronotypes. Numerous studies similar to our study did not find a significant relationship between chronotype and caloric intake [3,19,20]. For example, in the study of Kanerva et al. [20] conducted on 4,493 people aged 25–74, there is no association BMI, calorie intake, and MEQ questionnaire score. Similarity in total daily calorie intake of people with different chronotypes was mentioned as the reason of such finding. The same finding was obtained in the study of Toktas et al. [21]. The authors noted to this point that people with the eveningness type usually skipped at least one meal, which was mainly breakfast. But instead, the calories of this meal were usually compensated at dinner meal; whilst people with the morningness type, rarely skipped their meals. Therefore, total calorie intake of people with morningness and eveningness types was similar. In contrast, a study by Maukonen et al. [22] found that people with the eveningness type who intake most of daily calorie during the dark period (inactive phase) had a higher BMI than those with morningness type. It should be noted that the participants in our study had only overweight, not obesity; while the previous studies showing an association between chronotypes and BMI have been conducted on people with obesity [23]. It makes difficult comparison of our findings with theirs.
There is some evidences that food intake during the light period (active phase) may prevent obesity induced by high-fat diets through alteration of some metabolic pathways that occur in the liver [24]. These metabolic pathways depend on the biological clocks. Glucocorticoids are secreted from the adrenal gland in response to stressful stimuli and in response to the hypothalamic-pituitary-adrenal axis and act as powerful agents influencing on the many metabolic pathways, both in vitro and in vivo. Disruption or disturbance in the peripheral clock reduces the expression of period circadian regulator-1 through the glucocorticoid response element, which indicates that the coordination between the biological clock and the peripheral clock changes the secretory rhythm of adrenal hormones [25]. In addition, scheduled meal times reduce the circadian fluctuation of rhythmic genes and potentially reduce obesity due to high-fat diets. Also, exercise can be a useful and powerful tool for management of rhythmic patterns [26]. The results of the study by Gill et al. [25] showed that physical activity prevents obesity due to excessive calorie intake in light phase, but does not have such an effect on calorie intake in dark phase. Since there was no significant difference in physical activity level of participants with different chronotypes, assessment of its effects on calorie intake in different light cycles was not possible.
One of the remarkable points in the present study is that although the mean BMI of our participants was ≥25 kg/m2, the average calorie intake was lower than the amount expected for these people, according to their weight. Therefore, it is possible that the participants in the present study reported their food intakes lower than the real one. Under reporting of energy intake is common in overweight and obese people. Furthermore, the diversity of energy intake between participants were slight. So, lack of significant difference in energy intake of people with different chronotypes may be partly contributable to under reporting of energy intake.
Despite the similar distribution of BMI among different types of chronotypes, the percentage of body fat mass in people with eveningness type was significantly higher than people with morn- ingness type, while the percentage of muscle mass in people with morningness type was significantly higher than people with eveningness type. According to our knowledge, there are few studies conducted on the association between body composition and chronotypes. Furthermore, there is no study in this field in Iran. The study of Yu et al. [27], similar to our findings, showed that the percentage of adipose tissue in diabetic men with eveningness type is significantly higher than men with intermediate and morningness types. It may be explained by this fact that decrease in muscle mass is associated with increased insulin resistance, and lower muscle mass is more frequent in eveningnes type than two other types. The authors concluded that regarding the higher prevalence of sarcopenia in men than women in their study, more studies with a larger sample size are needed to examine the relationship between sarcopenia and chronotype in women. In addition, our findings are similar to the study by Soreca et al. [28], showing that the percentage of body fat in people with eveningness type is higher than people with other chronotypes. Generally, metabolic disorders are more associated with eveningness type than two other chronotypes. It can be attributable to the higher probability of insomnia in people with eveningness type and its detrimental effects on metabolic pathways [29]. Some studies show that people with the eveningness type suffer from sleep disorders more than others. Because the coordination between the sleep/wake cycles, which is regulated by the body’s biological clock, and the real time of asleep, which is regulated by social conditions, is poor in individuals with eveningness type [30-32]. On the other hand, poor sleep quality changes circadian rhythms and increases body fat mass through various mechanisms such as eating disorders and hormonal disturbance. Disorders of the body’s circadian systems affect not only on sleep quality, but also on appetite, energy expenditure, and some other metabolic components [33]. Late time meals reduce resting energy expenditure, thermic effect of food, glucose tolerance, and daily secretion rhythm of cortisol [34]. These metabolic changes may play an important role in increase in insulin resistance and the accumulation of adipose tissue in eveningness people. Furthermore, there are many genes expressed in adipose tissue following a circadian rhythmic pattern and so, circadian rhythm of these genes has a significant effect on adipose tissue [14]. On the other hand, muscle mass is an important organ for protein storage, glucose regulation, and myokin production, which can modulate insulin resistance and counteract the destructive effects of inflammatory adipokines [35]. Another possible mechanism that suggests an association between the eveningness type and metabolic disorders is related to the increased exposure to artificial light in the afternoon and evening. Exposure to light during inactive phase (dark cycle) reduces insulin sensitivity and increases inflammatory responses [36,37]. Therefore, eating at uncommon hours (inactive phase) may be associated with metabolic disorders which can see in people with the eveningness type [38].
Strengths and limitations
Among the strengths of the present study, we can mention the high sample size. One of the limitations of this study is its cross-sectional design; such that in these studies, exposure and outcome are examined simultaneously; so, it is not possible to comment definitively on the possible impact of exposure on outcomes. The second limitation of this study was the low job diversity among participants. Most of our participants were households or retirees. Also, because the participants in this study were selected from the community centers in Tehran, and considering that the official time of these centers is before the afternoon, most of our participants were housekeeper middle-aged women and so, the frequency of men was very fewer than women in our study. Energy underreporting was the other limitation which make difficult to find the association between chronotypes and food consumption.
Conclusion
The present study shows that in overweight adults, the eveningness type is directly associated with body fat mass and inversely with muscle mass. Further studies on a wider range of occupations and a more limited age range seems necessary to better understanding the association between chronotypes and obesity.
Notes
Funding Statement
None
The authors have no potential conflicts of interest to disclose.
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Author Contributions
Conceptualization: Samira Rabiei. Data curation: Samira Rabiei. Formal analysis: Hakimeh Sadeghzadeh, Mazyar Haghgoo. Funding acquisition: Samira Rabiei. Investigation: Hakimeh Sadeghzadeh, Mazyar Haghgoo. Methodology: Samira Rabiei. Project administration: Samira Rabiei. Resources: Hakimeh Sadeghzadeh, Mazyar Haghgoo. Funding acquisition: Samira Rabiei. Supervision: Samira Rabiei. Validation: all authors. Visualization: all authors. Writing—original draft: Hakimeh Sadeghzadeh, Mazyar Haghgoo. Writing—review & editing: Samira Rabiei.
Acknowledgements
We are grateful for the National Nutrition & Food Technology Research Institute, Shahid Beheshti University of Medical Sciences. We would also like to thank the community centers in Tehran and all participants in this study.