INTRODUCTION
Depressive episodes in major depressive disorder (MDD) and bipolar disorder (BD) are clinically different. In BD, atypical featuresŌĆöincluding psychomotor retardation, hypersomnia, increased appetite, sensitivity to rejection (which is more frequent with an earlier age at onset), and past histories of postpartum depression or psychotic featuresŌĆöare more often compared to MDD [1]. However, though these results are based on comparisons between groups, applying these results to individual patients is difficult [2,3]. Consequently, MDD and BD have the same diagnostic criteria for depressive episodes. Thus, many researchers have investigated biological differences between bipolar depression and MDD. They have considered using biomarkersŌĆöin blood specimensŌĆöHPA axis, oxidative stress, or molecular biology to help address this [4-9]. Additionally, loudness dependence of auditory evoked potential (LDAEP) to test serotonergic transmission was used to study the differential response to the treatment [10,11]. However, all the aforementioned biomarkers had limitations, with inconsistent results. Therefore, we aimed to use quantified electroencephalogram (QEEG) to differentiate BD from MDD [4-9].
The QEEG, now popular, has been used to investigate the neurobiological characteristics of depression, with many studies showing an increase in left hemispheric frontal alpha power in depressed patients compared to healthy controls [12-15]. Since alpha power is inversely related to neuronal activity, it reflects reduced activity in the left frontal region in patients with depression [16-18]. Studies have attempted to use alpha asymmetry as a biomarker in patients with depression [19,20]; however, such studies on alpha asymmetry remain inconsistent. We postulated that the inconsistency of frontal alpha asymmetry was because of the heterogeneous nature of patients with depression and the inclusion of patients with bipolar depression within the sample. Additionally, since frontal alpha asymmetry is related to cognitive function and neuronal activity, and cognitive dysfunction is more prominent in bipolar depression than in MDD, we postulated that frontal alpha asymmetry would be more prominent in bipolar depression. Some studies attempted to compare depressive episodes in BD and MDD using QEEG; however, little is known so far, with no decisive hallmarks differentiating the two [21,22]. In this study, we intend to use QEEG to directly compare the alpha asymmetry and absolute power of each band between patients with BD and MDD.
METHODS
Subjects and study design
A total of 50 in-patients with major depressive episodes were retrospectively enrolled. This enrollment, based on medical records at the Ilsan Paik Hospital between 2019 and 2021, included patients, aged 17ŌĆō71 years, diagnosed with either MDD (n=29) or BDŌĆötype I, II, or other specified bipolar and related disorder (n=21). Subjects who met the DSM-5 criteria for other major psychiatric disorders, such as schizophrenia or personality disorders, were excluded. The subjects were divided into MDD and BD groups according to DSM-5 criteria. QEEG recordings were collected, and self-reported questionnaires including Beck Depression Inventory (BDI), Korean version of Childhood Trauma Questionnaire (K-CTQ), Adult Attention-Deficit/Hyperactivity Disorder Self Report Scale (ASRS) were also used to collect clinical information. The BDI is a scale for measuring depression, which consists of 21 items with a three-point scale for each item [23]. We used the cutoff value for moderate depression, which was 20 [23]. Additionally, we also utilized the sleep-related item in BDI (item 16ŌĆö0: ŌĆØI can sleep as well as usual,ŌĆØ 1: ŌĆ£I donŌĆÖt sleep as well as usualŌĆØ, 2: ŌĆ£I wake up 1ŌĆō2 hours earlier than usual and find it hard to get back to sleep,ŌĆØ 3: ŌĆ£I wake up several hours earlier than I used to and cannot get back to sleepŌĆØ) to find out factors that were associated with insomnia with a cutoff of 1 or higher [23]. In the K-CTQ scale, all five subscales (sexual abuse, physical abuse, emotional abuse, physical neglect, and emotional neglect) were collected [24]. We used the cutoff values suggested by Bernstein et al. [24], the developer of CTQ. The ASRS was developed by Kessler et al. [25] and was used to screen adult ADHD; the first six items (Part A) were used in this study with a cutoff of 4, which is consistent with adult ADHD.
The study protocol was approved by the ethics committee of Ilsan Paik Hospital before beginning the investigation (ISPAIK 2021-08-055). Informed consent was waived because of the retrospective nature of the study.
QEEG and procedure
The E-prime software (version 2, Psychology Software Tools, Pittsburgh, PA, USA) was used to synchronize QEEG recordings and onset of stimulus presentation recordings. A Neuroscan SynAmps amplifier (Compumedics USA, El Paso, TX, USA) with 64 Ag-AgCl electrodes on a Quik-Cap was used to record the EEG in an extended 10ŌĆō20 placement scheme. The specific protocol has been described elsewhere [26,27].
The absolute power of the delta (1.0ŌĆō4.0 Hz), theta (4.0ŌĆō8.0 Hz), alpha (8.0ŌĆō12.0 Hz), beta (12.0ŌĆō25.0 Hz), and high beta (25.0ŌĆō30.0 Hz) waves, and the Z-scores of the alpha band wave asymmetry in the frontal lobe area were calculated with a confidence interval of 95%. The nodes for the frontal lobe area were FP1, FP2, F3, F4, F7, and F8, and asymmetry for FP1ŌĆōFP2, F3ŌĆōF4, F7ŌĆōF8 were calculated.
Statistical analysis
Participants were divided into two groups according to three categories: MDD vs. BD group, depression severity group (BDI Ōēź29 vs. BDI<29), ASRS positive (ASRSŌēź4) vs. negative (ASRS<4) group, based on the medical records and DSM-5. The groups were also divided by age (cutoff: 28, median value) and sex. Tests such as t-test and PearsonŌĆÖs correlation test were conducted. Analysis of covariance (ANCOVA) was also performed; this was based on the t-test and PearsonŌĆÖs correlation test results, with age and sex as covariates and diagnoses (MDD vs. BD) as fixed factors. The ANCOVA tests for the BDI and ASRS were included as fixed factors. In the ANCOVA test for BDI scores, age, sex, and ASRS scores were added as covariates. Age, sex, and BDI scores were added as covariates in the ANCOVA test for ASRS scores.
All tests were two-tailed, and the cutoff p-value for statistical significance was set at p<0.05. Statistical analysis was performed using SPSS software package (version 25, IBM Corp., Armonk, NY, USA).
RESULTS
Fifty patients were evaluated. The t-test was conducted by dividing them into two groups according to their clinical diagnoses (MDD and BD), age (cutoff: 28, median value), sex, BDI (cutoff: 20 [moderate] and 29 [severe]), and ASRS (cutoff: 4). The MDD group was significantly older (p=0.014), whereas the BD group had significantly higher physical neglect scores (p=0.044), a subscale of the K-CTQ. Older patients had higher right frontal alpha asymmetry at FP1ŌĆōFP2 (p=0.044) and F7ŌĆōF8 (p=0.021), with higher high beta power at FP1 (p=0.002), FP2 (p=0.005), F3 (p=0.019), F7 (p=0.025), and F8 (p=0.011). Women showed higher high beta power at FP1 (p=0.031), FP2 (p=0.021), F3 (p=0.003), F4 (p=0.041), and F7 (p=0.029). Men had higher physical neglect scores (p=0.015). Patients with moderate depression (BDI scores Ōēź20) had higher total K-CTQ (p=0.001) and emotional neglect (p=0.008) scores, and higher high beta and delta power at FP1 (p=0.017), F4 (p=0.002), F8 (p=0.013), FP2 (p=0.035), F3 (p=0.020), F4 (p=0.013), F7 (p=0.040), and F8 (p=0.040), respectively. Patients with severe depression (BDI scores Ōēź29) showed higher emotional neglect (p=0.021) and higher right frontal alpha asymmetry at F3ŌĆōF4 (p=0.036).
In the Pearson correlation test, physical neglect correlated with BDI (p=0.017, R=0.352), right frontal alpha asymmetry at F3ŌĆōF4 (p=0.044, R=-0.325), delta band power at FP2 (p=0.049, R=0.313), F3 (p=0.025, R=0.354), F4 (p=0.028, R=0.348), F7 (p=0.023, R=0.359), and F8 (p=0.036, R=0.332). Total K-CTQ scores correlated with right frontal alpha asymmetry at F3ŌĆōF4 (p=0.012, R=-0.396). Sexual abuse scores correlated with higher alpha band power at F4 (p=0.020, R=0.367). Age correlated with beta and high beta power at FP1 (p=0.039, R=0.316), F3 (p=0.049, R=0.301) and FP1 (p=0.000, R=0.542), FP2 (p=0.004, R=0.434), F3 (p=0.008, R=0.402), F7 (p=0.006, R=0.416), F8 (p=0.015, R=0.368), respectively.
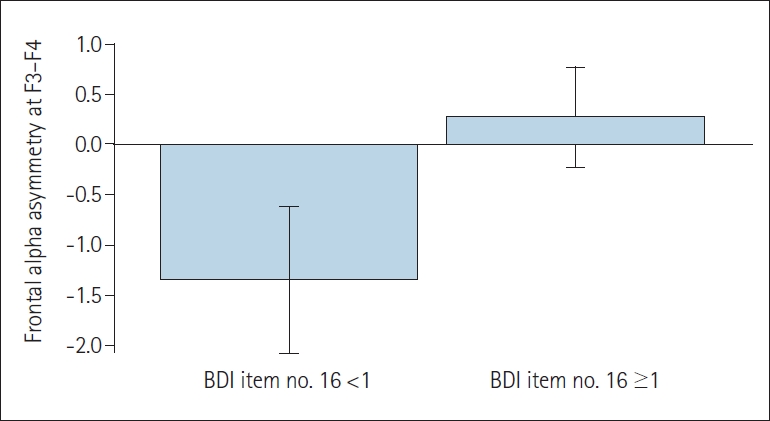
ANCOVA tests were performed based on the Pearson and t-test results. In the ANCOVA results, patients with BD had significantly higher physical neglect scores (p=0.027) (Table 1), but there were no other significant differences in band powers or frontal alpha asymmetry. Patients with severe depression (BDI score Ōēź29) showed higher total K-CTQ (p=0.008), emotional neglect (p=0.001), and physical neglect (p=0.035) scores (Table 2). These patients also had higher alpha power at FP1 (p=0.037), FP2 (p=0.028), F3 (p=0.047), and F4 (p=0.016). Right frontal alpha asymmetry at F3ŌĆōF4 was also prominent (p=0.039) (Table 2). Adult patients with symptoms consistent with ADHD (ASRS score Ōēź4) had significantly higher right frontal alpha asymmetry at F3ŌĆōF4 (p=0.046) (Table 3). For insomnia, the ANCOVA test was performed with the BDI score of item No. 16 as a fixed factor (0 vs. 1 or higher) and age, sex, ASRS, and BDI as covariates. The results showed that patients with insomnia had higher physical abuse scores (p=0.012) and left frontal alpha asymmetry at F3ŌĆōF4 (p=0.003) (Figure 1).
DISCUSSION
The current study revealed no significant findings differentiating between patients with MDD and BD, except for physical neglect scores. However, when focusing on the depression severity rather than the diagnoses, patients with severe depression had significantly higher alpha power at FP1, FP2, F3, F4, and right frontal alpha asymmetry at F3ŌĆōF4, with higher K-CTQ and physical and emotional neglect scores. Patients screened positive for ADHD showed significant right frontal alpha asymmetry at F3ŌĆōF4. Patients with insomnia had significantly higher physical abuse scores and left frontal alpha asymmetry at F3ŌĆōF4. In short, frontal alpha asymmetry was associated with cognitive symptoms, depression severity, and insomnia.
There have been few previous attempts to differentiate between MDD and BD patients using QEEG. Some investigators have attempted to differentiate MDD, BD patients, and healthy controls using EEG activity, and found that patients with MDD had significantly higher left frontal asymmetry compared to healthy controls; however, there were no significant differences in frontal alpha asymmetry in other comparisons [28]. However, other investigators have reported no differences in frontal asymmetry between MDD and BD [29]. Although our results did not fully discriminate between patients with MDD and BD, there were significant results when focusing on depression severity. One study revealed that alpha power increased, with higher left frontal alpha asymmetry in patients with MDD compared with healthy controls [30]. The same study also found that compared to patients with MDD without suicidal ideation, MDD patients with suicidal ideation had significantly lower left frontal alpha asymmetry, with reduced alpha power in the left frontal region [30]. Since suicidal behavior is a strong indicator of severe depression, this suggests that alpha asymmetry can indeed be meaningful in assessing depression severity. Conversely, our results showed right frontal alpha asymmetry in patients with severe depression. This is contradictory not only to the findings described above, but also to the conventional hypothesis that there is left frontal alpha asymmetry in patients with depression. This may be due to the heterogeneous nature of depression and inconsistent findings regarding the aforementioned hypothesis. However, because our findings are statistically significant, other factors, such as cognitive impairment, might have played a role in this result.
Several previous studies have shown a relationship between frontal alpha asymmetry and adult ADHD. A recent study revealed that ADHD symptoms meant significantly stronger relative right frontal alpha power in adults with ADHD [31]. In another study, patients with ADHD showed significantly stronger anterior cortical activity in the left hemisphere in adults [32]. An additional study also revealed the relationship between ADHD and frontal alpha asymmetry, suggesting that ADHD severity could be predicted by right frontal alpha asymmetry [33]. These findings were consistent with our results. However, one study reported left frontal alpha asymmetry in patients with ADHD, which is inconsistent with the findings discussed above [34]. Some studies have pointed out that worse ADHD symptoms meant significantly suppressed cognitive function [35,36]. Considering this, we suggest that a higher ASRS score can be interpreted as poorer cognition, and it is possible that cognitive impairment itself can contribute to frontal alpha asymmetry. Altogether, ADHD symptoms and cognitive impairment can both contribute to frontal alpha asymmetry.
Our results showed left alpha asymmetry in patients with insomnia. Attempts have been made to correlate frontal alpha asymmetry with sleep. One study found that sleep-deprivation induced significantly greater right-side alpha activation in the frontal region [37]. Another study revealed that frontal alpha asymmetry during wakefulness positively correlated with frontal alpha asymmetry during REM sleep [38]. Researchers have also found that dream anger can be predicted by right frontal alpha asymmetry during REM sleep [38]. Emotional dysregulation can contribute to insomnia, and lack of sleep itself can also affect left frontal alpha asymmetry [39]. Thus, the relationship between frontal alpha asymmetry and insomnia remains unclear. That may be due to the heterogeneity and confounders of depression that can affect QEEG results, such as education, medication, and handedness, could have accounted for these findings.
The current study has several limitations. This was a retrospective study, and the healthy control group was absent. Additionally, control for other confounders such as education, medication, and handedness was not considered. Patients with BD were mostly had bipolar II, with only two and one patients with bipolar I, and specified bipolar and related disorder, respectively. Therefore, our findings mostly reflected the aspects of bipolar II patients, rather than other types of bipolar disorders. Future research is required to address this issue. Despite this, the current study revealed that frontal alpha asymmetry did exist in depression and is affected by ADHD symptoms such as cognitive impairment, insomnia, and depression severity in particular. However, the current study suggests that QEEG, including frontal alpha asymmetry, has limitations in the differential diagnosis of MDD and BD. In future studies, methodological improvement with larger clinical samples or further control for confounders such as education, medication, and handedness would be necessary for better comparison.