INTRODUCTION
Insomnia, the most common sleep disorder, is highly prevalent. According to a study, chronic insomnia affects approximately 10% of the population, and around one-third of adults reports symptoms of insomnia without considering the duration [1]. Especially, the prevalence of insomnia is higher in elderly people than in the younger population, and in elderly, it ranges from 30% to 48%. A Japanese study estimated the annual economic loss due to insomnia to be around 3.5 trillion yen [2], while a Canadian study estimated a loss of 1.9 billion dollars per year [3]. Insomnia is also known to contribute to an increase in traffic accidents due to daytime sleepiness [4]. However, studies have shown that it can take 10 to 12 years for individuals with insomnia to seek professional medical help, underscoring the importance of diagnosing and treating this condition [5].
Current sleeping pills used for insomnia treatment have certain limitations including falling down, sedation, withdrawal symptoms, cognitive dysfunction, and hangover. To overcome these limitations, new drugs related to melatonin, a hormone involved in sleep regulation, have recently been introduced. Melatonin is a hormone that follows the circadian rhythm and is released by the brain to regulate sleep-wake cycles [6]. The newly developed drug is the first and only prescription drug that contains the prolongedrelease melatonin (Circadin®), distinct from the melatonin widely used as a sleep-related health supplement [7]. Although the efficacy of this drug may be slightly lower than that of existing sleeping pills, it poses no risk of dependence or withdrawal, as long as there are no dizziness or hangover symptoms the next day, which can occur with benzodiazepine hypnotics, nor any behavioral abnormalities associated with certain Z-drugs [8]. This drug has obtained approval from domestic clinical trial results and is currently being released in South Korea.
Therefore, the primary objective of this study is to evaluate the efficacy, tolerability, and potential side effects of the prolongedrelease melatonin in improving sleep quality.
METHODS
An 8-week prospective, open-ended, observational study was conducted on 115 patients aged 55 years or older with insomnia (age range: 55–90 years). Among all patients, 67 patients completed this study and 48 patients dropped out. The inclusion criteria involved patients who reported symptoms consistent with insomnia disorder according to the diagnostic classification criteria of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [9]. Additionally, patients with a Hamilton Rating Scale for Depression (HAMD) [10] score below 16 were included. The selection process also emphasized the importance of recruiting patients who were predicted to have good compliance with medication and demonstrated a cooperative attitude. The study excluded individuals with sleep disorders other than insomnia as per DSM-5 criteria, patients with other psychiatric disorders (except for mild depression with a HAMD score of 15 or less), and those known or expected to be hypersensitive to external melatonin or melatonin receptor agonists. Additionally, individuals with a history of drug abuse (including alcohol), the use of psychotropic drugs within the past 3 months, and the use of benzodiazepines or other sleeping pills in the past 2 weeks were also excluded. Baseline assessments, including the Pittsburgh Sleep Quality Index (PSQI) [11] and the WHO-5 Well-being Index [12] were measured at baseline. Subsequently, the prolonged-release melatonin (2 mg) was administered to the patients before bedtime. The sleep indices (PSQI, WHO-5 Well-being Index) were reevaluated at weeks 4 and 8 to determine improvements in sleep quality. The dosage of the prolonged-release melatonin remained at 2 mg throughout the study without any dosage escalation. Our participants consisted of two groups. One group received no hypnotics at baseline assessment, and another group had already received at least one type of hypnotics. Among 115 participants, one participant was excluded because of data unreliable. Finally, we used the data of 66 participants for per protocol analysis, and of 114 participants for last observation carried forward (LOCF) method.
Statistical analysis
Statistical analyses were performed based on per protocol analysis and LOCF method, and the data included all patients for whom at least a baseline measurement was available. The LOCF method was applied for endpoint analysis. All subjects who received at least one dose of the study medication were included in the safety analysis. In addition, second analysis was conducted using complete analysis. Categorical variables are presented as absolute numbers and relative frequencies (%) and nominal variables as means and standard deviations. Scores on each psychometric scale were analyzed by the Mann-Whitney U test, paired t-test, and repeated measures analysis of variance (RM-ANOVA). The Greenhouse–Geisser correction was used to test for non-sphericity in RM-ANOVA. The chi-square test or Fisher’s exact test was used to analyze categorical variables. All statistical tests were two-tailed with a significance level of 0.05. All statistical analyses were conducted using SPSS software (version 25, IBM Corp., Armonk, NY, USA).
Ethics
The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practices. Written informed consent was obtained from all subjects after they had been given an extensive explanation of the nature and procedures of the study. The study protocol was approved by the institutional review or ethics committees at each study site (ISPAIK 2015-10-001).
RESULTS
The study aimed to evaluate the effects of the prolonged-release melatonin treatment on various sleep parameters and well-being in patients with sleep disturbances. The analysis was conducted using two methods: per protocol analysis and LOCF analysis.
Per protocol analysis
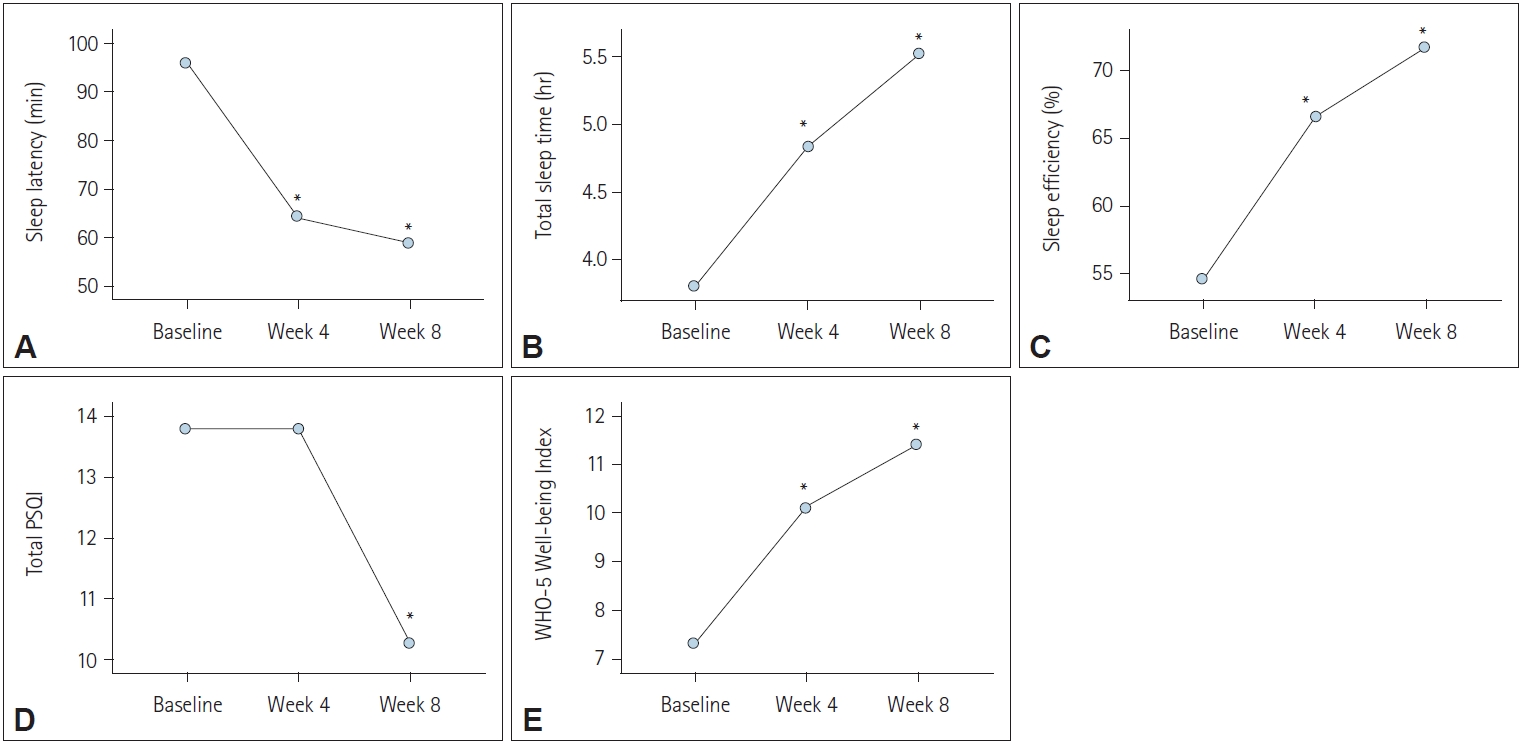
The results of the per protocol analysis indicated significant improvements in all five measured variables after 8 weeks of the prolonged-release melatonin treatment compared to baseline (Figure 1). Specifically, sleep latency and total PSQI showed a significant decrease over the 8-week treatment period, indicating that it took less time for patients to fall asleep, and their overall sleep quality improved (p<0.001) (Table 1 and Figure 1A, D). Additionally, total sleep time, sleep efficiency, and WHO-5 Well-being Index demonstrated a significant increase, suggesting that patients experienced longer and more efficient sleep and reported better overall well-being (p<0.001) (Table 1 and Figure 1B, C, E). When comparing the data at 4 weeks and 8 weeks of treatment with baseline, significant differences were observed in four of the five variables, except for PSQI (post-hoc test) (Table 1). These findings suggest that most of the improvements occurred by the 4-week and were sustained through the 8-week treatment period. Notably, the PSQI showed a significant difference only at 8 weeks, indicating that it might take more time for Circadin to have a noticeable impact on certain aspects of sleep quality.
LOCF analysis
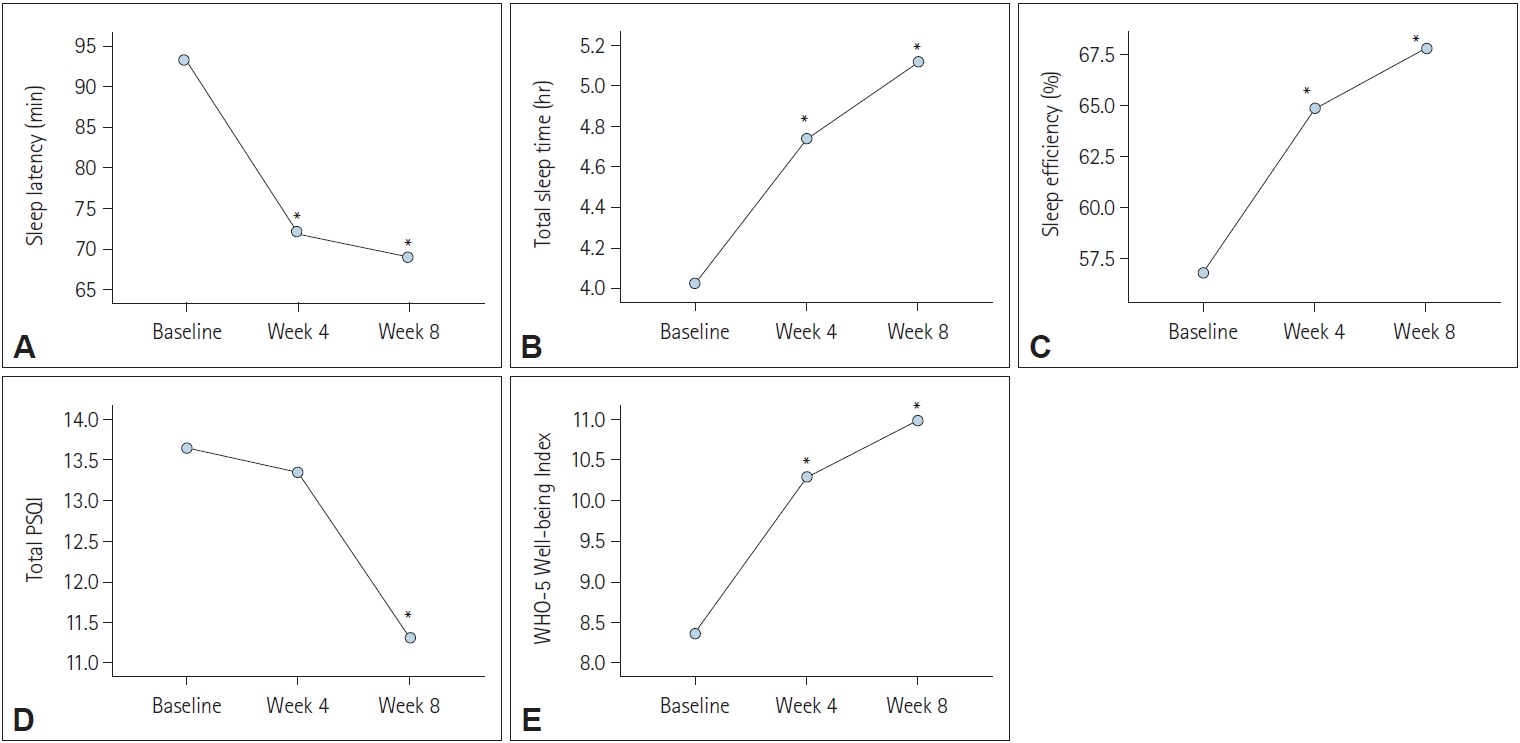
The LOCF analysis provided results nearly consistent with the per protocol analysis. After 8 weeks of Circadin treatment, all five variables showed statistically significant differences compared to baseline (Figure 2). Similar to the per protocol analysis, sleep latency and total PSQI demonstrated a significant decrease over the 8-week period, indicating improved sleep initiation and overall sleep quality (p<0.001) (Table 2 and Figure 2A, D). In contrast, total sleep time, sleep efficiency, and WHO-5 Well-being Index significantly increased, indicating longer and more efficient sleep and improved well-being (p<0.001) (Table 2 and Figure 2B, C, E). Like the per protocol analysis, significant differences were observed at 4 weeks and 8 weeks when compared to baseline, except for the PSQI variable, which showed a significant difference only after 8 weeks of treatment (Table 2).
Safety
During the study period, a careful assessment of adverse events associated with the prolonged-release melatonin treatment was conducted. Table 3 provides a summary of the observed adverse events. Among the reported adverse events, dizziness and heartburn were the most frequently encountered, with each occurring in three cases. Additionally, one instance of insomnia aggravation, headache, and dyspepsia was documented.
Dropout and discontinuation
A notable aspect of the study was the dropout rate, which occurred in 48 out of 115 participants, representing a dropout rate of 41.7%. The reasons for dropout varied and included follow-up loss, discontinuation due to lack of efficacy, and discontinuation due to adverse events. Among the participants who dropped out, 21 individuals were lost to follow-up, which accounted for a significant portion of the total dropouts. Additionally, 19 participants discontinued the study due to perceived lack of efficacy, indicating the challenges some participants faced in experiencing the desired outcomes from the treatment. Furthermore, 8 participants chose to discontinue the study due to adverse events. These adverse events may have contributed to their decision to withdraw from the study prematurely.
DISCUSSION
The present study sought to assess the efficacy, tolerability, and safety of the prolonged-release melatonin in improving sleep quality among elderly patients with insomnia. The results of this study provide valuable insights into the potential benefits of the prolonged-release melatonin in addressing the sleep disturbances commonly experienced by this patient population.
Efficacy and sleep improvement
The findings from both per protocol and LOCF analyses demonstrated consistent improvements in various sleep parameters and well-being following the prolonged-release melatonin treatment. Notably, sleep latency significantly decreased, indicating that patients experienced faster sleep initiation after 4 and 8 weeks of treatment. This improvement is in line with the results of a study which similarly reported a reduction in sleep latency among elderly individuals treated with the prolonged-release melatonin [8]. Total sleep time and sleep efficiency also improved significantly, suggesting that patients experienced longer and more restful sleep. These findings are consistent with a randomized controlled trial, where the prolonged-release melatonin was associated with improved total sleep time and sleep efficiency in elderly patients with insomnia [13]. The observed increase in the WHO-5 well-being index underscores the positive impact of the prolonged-release melatonin treatment on patients’ overall sense of well-being, which demonstrated improvements in well-being following melatonin treatment [8]. The safety profile of the prolonged-release melatonin appears promising, with the most commonly reported adverse events being dizziness and heartburn. These adverse events were generally mild and manageable, consistent with the findings of a study which reported similar adverse events in elderly patients treated with the prolonged-release melatonin [7]. Importantly, no significant concerns regarding dependence, withdrawal, or behavioral abnormalities were observed, further highlighting the potential advantages of the prolonged-release melatonin over traditional sleep medications such as benzodiazepine hypnotics and certain Z-drugs. These safety considerations are particularly relevant in the elderly population, where drug interactions and side effects can pose significant challenges, as noted in studies [14]. The study’s dropout rate of 41.7% is noteworthy and highlights some of the challenges faced by elderly patients in adhering to insomnia treatment regimens. This high dropout rate aligns with previous studies where dropout rates in insomnia trials involving elderly individuals have been commonly reported [15]. Factors contributing to dropout included followup loss, perceived lack of efficacy, and adverse events [16]. However, it is highly likely that the dropout rate was high in this study due to a lack of efficacy. This is because the frequency of adverse effects in per protocol analysis was very low, and 61% of the subjects complained of insomnia even though they were already taking sleeping pills, so they can be seen as treatment-resistant patients.
The distinct advantage of the prolonged-release melatonin lies in its sustained-release formulation, which provides a more physiological mimicry of the natural circadian rhythm of melatonin secretion [7]. While the efficacy of the prolonged-release melatonin may be slightly lower than that of traditional sleeping pills, its favorable safety profile and potential for sustained benefits make it a promising option, especially for elderly patients who may be more susceptible to adverse effects and drug interactions, as emphasized in the studies [17,18].
Limitations and future directions
Several limitations of the study should be acknowledged. The high dropout rate raises questions about the generalizability of the findings to the broader population of elderly patients with insomnia. Additionally, the study’s duration of 8 weeks may not capture long-term effects or potential changes in efficacy over extended periods of use. Further research is warranted to explore the longer-term effects of the prolonged-release melatonin and its potential for preventing relapse after treatment discontinuation [17].
Conclusion
The present study provides valuable evidence supporting the efficacy, tolerability, and safety of the prolonged-release melatonin, a sustained-release melatonin drug, in improving sleep quality and overall well-being among elderly patients with insomnia. The observed improvements in sleep latency, total sleep time, sleep efficiency, and well-being align with findings from previous studies, highlighting the potential benefits of this novel treatment approach. While challenges such as a high dropout rate and individual variability in treatment response exist, the prolonged-release melatonin holds promise as a valuable therapeutic option for addressing the sleep disturbances experienced by the elderly population. Further research, building upon the contributions of prior studies, is needed to refine treatment strategies, enhance adherence, and establish the long-term benefits of the prolongedrelease melatonin in this clinical context.